


I’m super underslept, but it’s not like I don’t have valid reasons. It seems that there aren’t enough hours in the day anymore. This is without riding, which usually takes up the biggest chunk of time of my day.
I’ve been working on this bathroom most of my waking hours. My time day rotated to 4 am yesterday morning, which means that yesterday was over almost by the time I woke up. It takes a lot of thinking before there is any doing in this project. The building is 125 years old and everything is a little out of whack. Anyway, it is slowly getting there.
I took time to watch most of the Royals game last night. It happens that it was on Tuesday night beer ride, which makes it hard to get back to work after. They only had beer that had at least 7% alcohol, so it got a little ugly. I left after a couple beers to go eat at the Burgerstand and watch the rest of the game. It was already 8-0 Royals by that time. So, it comes down to game 7 tonight.
There is talk about driving down to Kansas City to the Power and LIght District or the Plaza, for tonight’s games, but I’ll have to see how the day goes. That would probably get real long, like tomorrow long.
Okay, below is the blood test results from a friend. Check out the hematocrit and hemoglobin numbers. Also the MCV. What’s up with these numbers? Maybe JV if he’s reading this could pipe in with his ideas. He is an expert on blood values. Anyone else have any ideas about these crazy numbers?
Okay, I need to get going. Physical therapy again this afternoon. Part of that is sort of an upper leg massage thing, but it always comes first. I told Burt last time that I’d like the massage after the PT exercises, not before. We’ll see if he rotates the schedule.
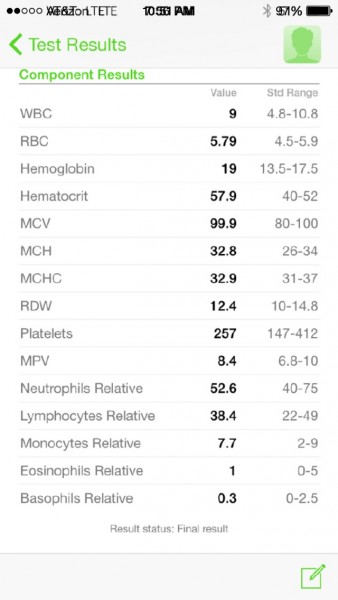
Blood test. Dehydration doesn’t explain these numbers.
Smear by the Royals last night in the World Series.
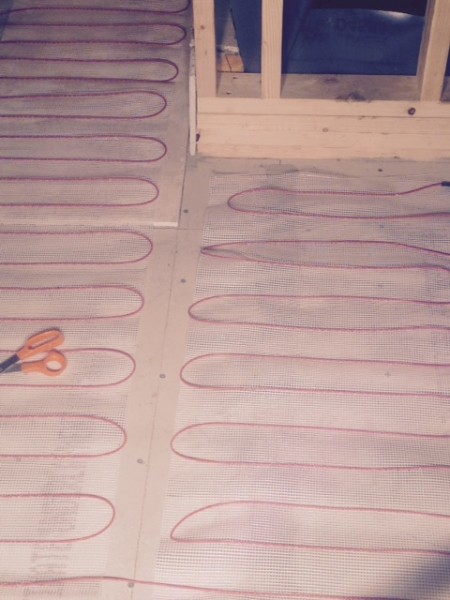
In floor heating mat.

I’m using 18 x 18 tile. It takes a ton of thinset.

I found this old t-shirt in the grout cleaning rag pile. Fresca for cycling, yum.

I’m putting in a baby sink. The whole space is only 6 foot by 6 foot.

The Insight has turned into the work truck. It doesn’t much like weight.

Finished shower pan.
Love Fresca! Only the original grapefruit variety though.
I think it’s funny that 52% is considered the upper std limit for hematocrit. Didn’t the UCI make you sit-out for “health reasons” if you went above 50? Would 52% trigger a bio-passport violation today?
Your ‘friend’ is cheating . . .
Drove by a Quality Inn on the way to work, so this is more of a guess on the blood values. The person tested is a male, and a teenager. May have been slightly sick, but not allergy related. Hematocrit and Hemoglobin values appear high for an Adult, but are possible on an athletic teen. Altitude could also be an additional component to the teenage aspect.
My guess would be lab error. It happens from time to time. In a health care setting they’ll typically re-test to rule out lab error before they do other (more costly) testing. If they get the same result on the second lab test, then they would probably look further for the cause.
well, since it’s my blood test I’ll chime in, I am not an athletic teen. I’ve always put up high numbers, 50-52 is pretty normal for me. No kidding, this goes back years. My blood pressure is low, 120/70 or so, used to be lower when I was fit, I’m not very fit. I have mild sleep apea and have not been using my cpap. I do not think I was dehydrated day of the test. Stress could have been a factor. I’m 51. The test was done on a friday and the two weeks leading up to the test I had been really sick with an upper respiratory infection and had been on antibiotics and prednisone, the does where you take 6 then 5 then 4 etc, I called the doc today and they are going to retest. He also asked what my Sherpa name was.
Corticosteroids increase RBC and hemoglobin: http://www.ncbi.nlm.nih.gov/books/NBK13780/
It’s for sure the prednisone.
Do you smoke? Just like altittude the carbon monoxide and lack of o2 will jack harmatocrit up quick
Not sure if you have done radiant heat before, but the bigger the tile, the better. small tile will have more grout which does NOT heat up. You need big tiles to get max warmth.
Was a reticulocyte count performed? Chronic hypoxia (sleep apnea) could stimulate EPO release from the kidneys and increased RBC production, kind of like sleeping in an altitude chamber or the secondary polycythemia seen with Pickwick Syndrome.
You should definitly go to KC. It may be another 30 years before the Royals make it to the Series again. GAME 7 WORLD SERIES – NO BRAINER!!
I sure hope the USADA/UCI doesn’t come knocking on your door, Steve , I mean Steve’s “friend”…
Considering that Steve is posting a screenshot taken on one phone and sent to another, probably his, I’d say it is a friend. Or Steve’s phone works on both AT&T and Verizon networks simultaneously, at different times of the day.
What? I always have screen shots of my friend’s blood tests. Don’t you?
just about everyone of your posts is doping related.
Just about everyone of your comments is dumbass related.
The steroids will jack the hemoglobin.
I was looking at this exact issue today and found this post by a MD:
I’m an Anesthesiologist and ICU MD (basically a clinical physiologist), not an exercise physiologist but I think there’s quite a bit of crossover. So I will post in this viper pit for the first time. If you find it mundane or irrelevant, please skip my post and accept my apologies.
First off regarding your athlete’s Hct. Highest likelihood would be a false result. That happens in my practice fairly frequently. If a lab test seems very out of whack, it’s probably spurious. A simultaneous Arterial Blood Gas should show concomitant metabolic acidosis or else something is up. If I saw that I would send a recheck, then agressively re-hydrate her until she’s peeing clear and copious and re-check again. If ABGs show that metabolic acidosis has normalized through hydration and the crit is still in the 60s, then she needs to be evaluated and phlebotomized. Anyone who gets into the 60s through fluid losses alone should feel like total crap, like crawling on all 4s down Alii Drive crappy. If her crit remains in the 60s with evidence of adequate intravascular volume status (not dehydrated) then she is in danger of an ischemic event and needs to be bled, Renaissance style. That’s what I would do, but I can get a crit, ABG and lactate level every 5 minutes if I want to. I realize that’s not the real world of athletics in the field.
If it turns out your athlete is doping, take her to a NeuroICU and show her a patient who has stroked out their Circle of Willis and can barely move, eat or talk ever again. Tell her that a true, sustained crit of 62 could easily get her a bed right next to that patient, not years from now, but hours from now. Then ask her if it’s worth it.
That being said, I have always been concerned about the value placed on random, occasional hematocrits in the fight against doping. It is not at all uncommon to see a patient’s crits fluctuate up and down during surgery or an ICU stay, even without bleeding, transfusion or EPO. There’s a lot more in the bloodstream than just red cells. It’s just a matter of hemoconcentration or dilution. We can make the crit go up 10-12 points in hours without transfusion or EPO (that’s way too short of a time frame to make red cells anyway). A higher crit DOES NOT necessarily mean more red cells or oxygen transport in the body at large. Any fluid losses without bleeding can get your crit up. Diabetes Insipidus is a classic example. If we’re not careful the crit can become quite high, and I assure you those people aren’t doping.
The point I’m trying to make is that crit is not even close to an absolute factor. It goes up and down relative to fluid and hydration status hour by hour. If you take a crit at the end of a 2+ hour long, hot run without fluids you will get a high value. Let that person hydrate for 3-4 hours and you can get a much lower number. Certainly within the range 10-12 points change, I believe. This is why I’ve never been comfortable with the randomly chosen crit of 50% to define someone who “must be cheating”. I always wonder, what were the circumstances when that crit was drawn? I need more data to say something like that and this is all I do 80 hours a week for the past 10 years. Even the Biologic Passport does not approach the number of samples over time I believe one would need to get a reliable sense of a person’s natural trends and fluctuations. It’s not uncommon for me to see dozens, even hundreds of crit values on a patient over time. After gathering all that then yes, I believe an outside observer could graph them out and say “something fishy changed at this time HERE. DOPAGE!!!!”. I don’t think the doping authorities are coming to every athlete’s houses 2-3 times per day.
You may argue that the OR or ICU represent extremes of human experience that don’t relate to exercise physiology and in the case of my running (or most people on these boards) I agree. But I believe the TDF, Ironman, or 2:03 marathon represent human physiology at an extreme equal to many surgical experiences or ICU stays.
I fear the whole strategy of non-positive doping investigation is unsound and frequently tragic. Spot-checking physiologic parameters of mutants who dance around the extremes of normal human physiology on a daily basis and comparing to normal values or randomly drawn lines in the sand seems like grasping at straws and ripe for injustice. It frankly seems a bit pathetic. I realize the authorities are battling substances and techniques that they may not even know about yet and there won’t be a true chemical ID test for every substance, but what happened to good, old-fashioned police work? I can’t care for a patient in the most simple way without producing Hefty Bags full of garbage and medical waste. It’s quite ridiculous and wasteful. This is not ambiguous garbage. Frequently soiled with blood, toxic, and easily identifiable by a lay person from 100 yards away, I would imagine. In fact, when health care worker are caught diverting and using medical narctoics, they are almost always given away by their paraphernalia and disposal attempts rather than a positive drug test (“uhhh, why do you need to have used syringes in your locker?!?”).
If I was a French journalist, my daily mission in life would have involved doing whatever is necessary to stalk and sort through Lance Armstrong’s garbage and the garbage of every place he goes for the 4 months that led up to any his TsDF. I can’t believe that any disposal scheme, no matter how elaborate and well-executed could have made every syringe, needle, vial, IV tubing, etc just disappear into the ether. All together over 8 years in pro cycling it would probably fill a garbage barge. I don’t know which idea I find more incredible: that Lance was the only one NOT doping, or that NO ONE has ever found ANY leftover paraphernalia that either tested positive or was ridiculously suspicious enough to make his sponsors bolt. Especially when doing so would make you into the French equivalent of Woodward and Bernstein, the hero of the TDF and an entire nation.
Read more: http://www.letsrun.com/forum/flat_read.php?thread=4077008&page=2#ixzz3Hc2q76yR
Hmmm. Could his RBC, hematrocrit, hemoglobin not be related directly to just having taken prednisone?
Did I stumble into a med school class?
Secondary polycythemia most likely. Doubt Polycythemia vera (which is a myeloproferative disorder) due to the fact the platlet count is normal. The work up should include a EPO level, and JAK-2 test. The most likely explanation is poorly controlled sleep apnea which result in prolonged periods of night time hypoxemia. There are times when phlebotomy can help with symptoms if they are there. See a hematologist.
They should have waived Gordon through and sent him to home last night in the ninth inning.
Yep. Not the first screw up by the coach there. KC habit of waiting for stuff to happen bit them in the ass.
Oh, wait, its bottom of the ninth?!?!?!?!
Last year a friend, early 50’s, was diagnosed with bone cancer. Elevated hematocrit, low 60’s, was what they started to look into after a routine physical. This in’t anything to play with, especially at your age. Get yourself checked out.
And he would have been out by 10 feet.
they made you sit out over 50%, but you could get a special dispensation if you could prove >50 was natural for you. A small number per year (3-5 iirc) were able to prove this.
I’m curious to find out what blog system you’re working with?
I’m experiencing some minor security issues with my latest blog and I’d like to find something more safe.
Do you have any suggestions?